ABDOMINAL AORTIC ANEURYSM

AIMS
Understand the indications for AAA PoCUS
Identify the normal abdominal aortic and vascular anatomy
Be able to image the abdominal aorta in short and long axes from the diaphragm to the bifurcation
Be able to take accurate measurements of the abdominal aorta in 2 planes at the proximal, mid and distal aorta
Be able to recognise aneurysmal change in the aorta
Be able to recognise limitations of bedside aortic ultrasound and potential pitfalls
EPIDEMIOLOGY
The prevalence of AAA ( >/= 3cm in size) is probably around 5-10% in men aged 65-79 yrs and about 1-2% in women (Jones et. al. 2016).
The mortality rate from a ruptured AAA is around 90%, with less than 50% of those with an acute rupture making it to hospital.
In New Zealand mortality for those receiving emergent AAA repair (many do not receive operative care) is around 35% compared to an elective repair mortality of 7% (NZMJ) 2012).
Mortality increases with age
Maori experience AAA events at a younger age, with an event rate 1.5 times NZ Europeans, and a mortality around twice that of NZ Europeans (NZMJ 2012)
RISK FACTORS for AAA
Older age (Younger in NZ Maori men and women)
Male
Cardiovascular disease
Risk increases with burden of cardiovascular disease
Risk of AAA at a younger age
Smoker past or present
Hypertension
Family history
CLINICAL PRESENTATIONS OF AAA
Ruptured AAA can present in a myriad of ways. Less than 50% of patients present with the classic triad of hypotension, pulsatile abdominal mass, and back/abdominal pain.
Emergency doctors should have a low index of suspicion for AAA especially in the middle/older age groups.
Complications of AAA include:
Rupture usually with pain
retro-peritoneal - may be relatively more stable, may extend
intra-abdominal with shock
Dissection
pain
organ ischemia
limb ischemia
Thrombo-embolic event
limb ischemia
distal embolic events
Aorto-enetric fistula (rare)
SIGNS AND SYMPTOMS
Collapse or syncope
Hypotension and shock
Back and or abdominal pain
Pulsatile abdominal mass - sensitivity only 68% (Fink et. al. 2000)
Flank pain - renal colic mimic
Limb ischaemia, pulse deficits, and embolic events
Non specific back pain (usually non mechanical in nature)
Sciatica mimic
Massive GIB (aorto-enetric fistula)
AORTIC and iliac ANEURYSM

Abdominal:
A normal abdominal aorta is 2cm or less
Conventionally an aneurysm is diagnosed when the abdominal Aortic diameter exceeds 3cm or more.
There are two main types of aneurysm fusiform (the most common) and saccular.
The majority occur in the mid-distal aorta
Surgically defined in relation to renal arteries as infra-renal (90%), juxta-renal, or supra-renal
When involving the distal aorta they may extend into the iliac arteries (10-20%)
Iliacs:
Isolated iliac aneurysms account for only 2% of abdominal aneurysms
70% of these are the common iliac artery (CIA)
30% Bilateral
CIA > 2.5cm is considered high risk
Male > 1.7cm is abnormal
Female > 1.5cm is abnormal
Risk of rupture:
Risk of rupture for a AAA is dependent on the size and also the rate of growth
small aneurysms can rupture !
< 4cm has a 5yr rupture risk of around 2% (AHA)
> 5cm the 5yr rupture risk is 25% (AHA) - risk increasing with size
INDICATIONS FOR AAA POCUS
Bedside ultrasound for AAA is indicated whenever there is clinical suspicion for AAA (see above).
Usually incorporated with bedside imaging for free fluid in the abdomen in the unwell patient.
Risk factors, signs or symptoms for AAA
Unstable patient not suitable for transfer to CT
Setting of undifferentiaed shock
It is an effective, highly accurate, and sensitive tool when carried out in the correct manner:
Early detection of AAA in the ED can significantly reduce mortality (Costantino et. al. 2005)
CT is gold standard but is often not safe or feasible in the unstable or undifferentiated shocked patient
PoCUS for AAA has a sensitivity of 99% and specificity of 98% (Rubano et. al. 2013)
LIMITATIONS
Patient and other factors may limit imaging completeness or interpretation
User dependent
Limited imaging of any potential retro-peritoneal rupture
Cannot exclude secondary or other complications such as dissection, organ infarction etc.
Any new abnormal bedside abdominal aortic ultrasound finding should be discussed with a senior ED doctor, and consideration for a CT made.
Even with an apparently normal bedside aorta scan, if there is significant clinical suspicion for aortic pathology a CT should be carried out.
anatomy of the aorta

The Aorta passes through diaphragm at T12 the level of the xiphoid process. It runs to the left of the midline anterior to the vertebral bodies before bifurcating approximately at L4, the level of the umbilicus.
Proximal aorta: Diaphragm-celiac-SMA
Mid aorta: SMA to renal arteries
Distal aorta: Renal arteries to bifurcation
MAJOR branches FOR POCUS
Celiac Trunk
Just below diaphragm
Common hepatic and spleenic arteries arise off the trunk - Seagull sign
Superior Mesenteric Artery (SMA)
1cm below celiac trunk
Runs anterior and parallel to aorta in caudal direction
Good point for a “suprarenal measurement”
Renal Arteries
Distal to SMA
Usually not seen in sagittal views
<3cm from diaphragm
90% of aneurysms originate distal to this point
ABDOMINAL AORTIC POCUS
Introduction to bedside Abdominal Aorta Exam
Introduction to Abdominal Aorta Focused Ultrasound Examination - Jason T Nomura
PREPARATION
Machine:
Curvilinear probe with lots of gel
Abdominal preset
Initial depth setting around 15cm
Patient:
supine
if feasible knees up can relax abdominal muscles
INITIAL ORIENTATION TO THE ABDOMINAL AORTA
Start at the epigastrium in the transverse plane (short axis of the aorta) with the probe marker to the patients right side. Use the liver as a sonic window to help attain image.

Source: POCUS 101
Short axis proximal abdominal aorta
Source: Core EM
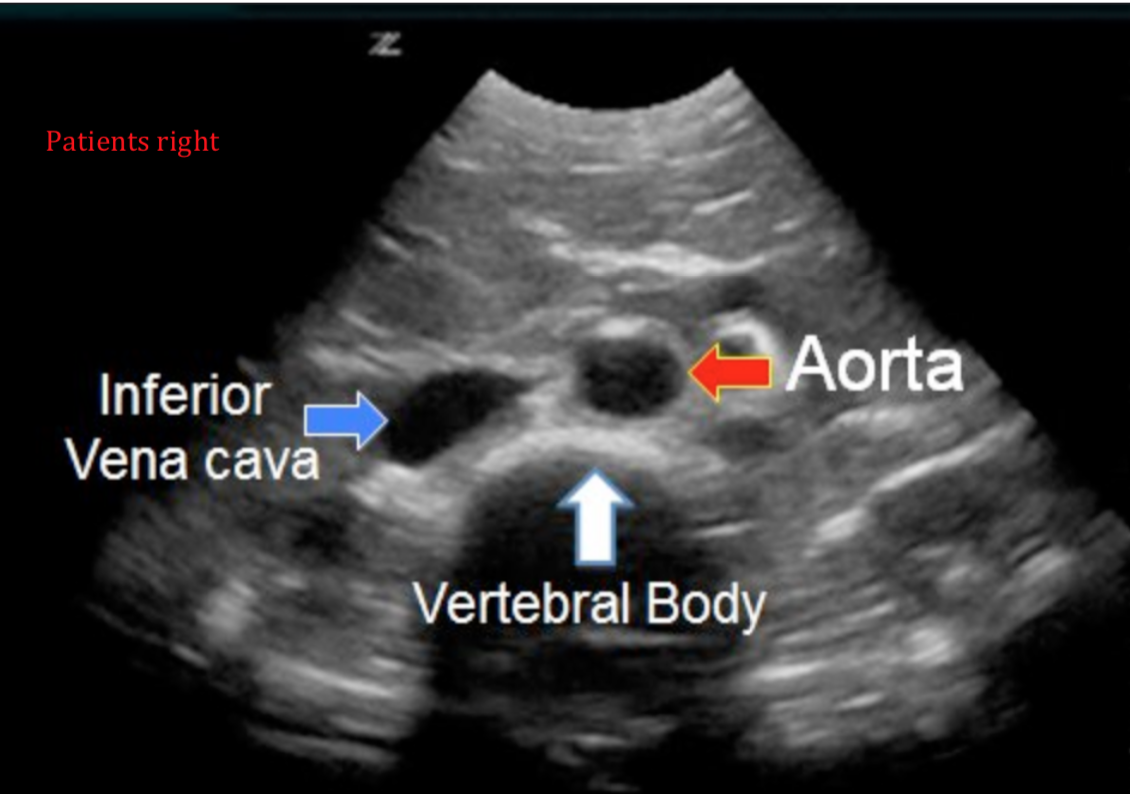
Identify the vertebral body
Identify the aorta:
Superficial to the vertebral body slightly to the patients left
To the right of the midline on the screen (check probe marker orientation)
Circular in the short axis
Pulsatile
Thick walled
Identify the IVC
To the left of the midline on the screen - the patients right side
Less circular
Usually displays collapsability with respiration
Optimise the image:
Depth - reduce depth so that the vertebral body is just at the bottom of the screen
Gain - adjust gain so that the aortic lumen is relatively anechoic (black)
Focus - ensure focus is at the depth of the aorta
Long axis localisation of the aorta:
If difficulties localising or differentiating the aorta in the short axis the probe can be rotated into the long plane at the epigastrium (probe marker to the patients head)
Tilt the probe keeping it at the midline sweeping from the patients right to left

Long axis proximal abdominal aorta
IVC seen to the patients right side passing in close association with the liver receiving the hepatic vein, before passing through the diaphragm into the base of the heart.
Aorta seen slightly to the patients left side identified by the branches SMA and celiac
Sitting anterior to the vertebral bodies
Seen by rocking the probe cephalad, the most proximal extent of the the abdominal aorta will dive deep to the liver passing behind the diaphragm
Continue imaging of the aorta (see protocol) from this point in an ordered sequence imaging the aorta in short axis and then long axis. Taking measurements in both planes at the proximal, mid, and distal aorta down to the bifurcation. Ideally the right/left CIA should also be imaged and measured.
ABDOMINAL AORTA PROTOCOL
SHORT AXIS
Start in the short axis (transverse plane) and identify the aorta:
An initial short axis scan from the xiphoid level distally down to the aortic bifurcation can be done to get a general impression
A video clip may be taken of this
Measurements of the aorta in short axis should be made in the transverse (Tx) and anterior-posterior (AP) dimensions at the proximal, mid and distal aorta.
Must be outer wall to outer wall
Images should show the maximal dimension of the aorta at that level i.e. measure the largest dimension seen
Save images at each identified important anatomical level with measurements

Source: EM Curious
Proximal Aorta
Locate the aorta at the epigastrium, as described above, in the transverse probe orientation:
Idenitfy the ‘SEAGULL SIGN’ made by the celiac trunk branches the hepatic and spleenic arteries
The celiac trunk may be hard to see - tilt the probe cephalad to help
Slide down distally to identify the SMA a small circle sitting superficial to the aorta
Just distal to the SMA origin, the left renal vein may be seen passing across the midline between the SMA and aorta to enter the IVC
The spleenic vein passes across the midline superficial to the SMA to the venous confluence which forms the portal venous system.
Measure the short axis proximal aorta at the largest dimension between the celiac and SMA (AP and Tx measurements)

Source: ultrasoundidiots.com (modified)

Source: Taming the SRU
Mid Aorta
This is the SMA down to the level of the renal arteries. The renal arteries can be hard to identify so measurements are taken just below the SMA origin
Renal arteries often < 1cm from SMA origin
90% of AAA are infra-renal (below renal arteries)
Involvement of the renal vessels has surgical consequences but is not an important part of your PoCUS exam
Measure the mid aorta short axis just below the SMA origin, if identified measure dimensions at the level of the renal arteries

RIGHT AND LEFT RENAL ARTERIES ARISING OFF LATERAL WALLS OF THE AORTA - Indicated by right and left artery notation in the image
Source: Sonosite

Distal Aorta
This is below the renal arteries to the aortic bifurcation:
Scan down until the bifurcation is noted
Measure the largest dimensions noted proximal to the bifurcation
LONG AXIS
Start again in the epigastrium turn the probe 90 degrees clockwise from the transverse orientation to the long axis (probe marker towards the head).

Attain an images from the most proximal aorta (near diaphragm) down to the bifurcation:
Often can be attained in 2 images
Elongate the aorta by rotating the probe slightly to attain the the best/most complete long axis view (opening up the long axis view)
Ectatic aortas can be hard to fully visualise across the long axis length so manipulation of the probe may be required to attain dimensions at each level.
Identify celiac and SMA
Ensure visualisation down to bifurcation, normal tapering (smaller dimension) of the aorta should occur

Source: Ultrasoundidiots.com (modified)
Measure AP dimension at proximal, mid and distal aorta
Measure outer wall to outer wall
Measure perpendicular to the walls
Ensure in the midline of the long axis of the aorta
A measure off the midline will underestimate the AP dimension
This is the cylinder tangent effect (below)

Lema (2017) Cylinder Tangent Effect
COMMON ILIACS
If possible the common iliacs should be included in your beside aorta ultrasound
Up to 20% aortic aneurysms extend into the iliacs (unilateral or bilateral)
Iliac aneurysms account for 2% of primary aneurysms of aorta of which 70% involve the CIAs
> 1.5cm female abnormal
> 1.7cm male abnormal
Ideally measure in short axis (AP + Tx dimension) and long axis (AP dimension)
Short axis view:
Starting at the distal aorta scanning distally until the aortic bifurcation into the right and left CIAs.
Measure the AP and Tx dimension

Source: Gulf Ultrasound

Source: Core EM (Modified)
Long axis view:
This can be attained from rotating the probe perpendicular from the short axis view of the each CIA, or by using a coronal view of the aortic bifurcation.
From the short axis probe position for each CIA
R CIA - rotate the probe clockwise to the long axis, probe marker cephalad to patients left
L CIA - rotate the probe clockwise to the long axis, probe marker cephalad to patients right
Care is required not to confuse the common iliac veins (CIV) with the CIA which can be seen running parallel
Colour Doppler can be used to determine directionality of flow to distinguish between the two (Probe marker must be toward patient head)
Coronal view of the CIA
Identify the level of aortic bifurcation (usually the umbilicus) from normal midline short axis view
Place the probe in a coronal position at the identified level (probe marker to the head)

Sources: Philips Ultrasound/Gulf Ultrasound
TROUBLE SHOOTING ABDOMINAL AORTIC VIEWS
Aortic views can be hindered by a number of issues. The most important of these being bowel gas and significant abdominal obesity. A number of techniques, and alternative sonographic windows can be utilised to help attain views.
Bowel gas
Often encountered in the upper abdomen causing dirty shadowing

Source: POCUS 101
Techniques to overcome bowel gas:
Utilise the liver as a sonic window to help visualise the proximal/mid aorta
A deep breath hold can help bring the liver down to increase your window
Graded constant downward pressure at a static probe position (check patient comfort) applied for a few minutes can help disperse the bowel gas
Left para-midline short/long axis views
Probe placed to left of the midline and angled towards the aorta
Start imaging distal and return to the proximal aorta, bowel gas can often disperse over time
Position patient in left lateral decubitus and scan in usual planes
Coronal plane ALTERNATE WINDOWS to the abdominal aorta
Due to bowel gas or obesity sometime alternate windows may be required to visualise the aorta. The most common being right or left coronal views, using the liver or spleen as acoustic windows.
Limited to single axis measurement
Often only visualise proximal portion of the abdominal aorta

Source: POCUS 101 (Modified)
OBESITY
Sometimes significant abdominal obesity can limit visualisation, a number of methods can help to identify the aorta.
Place patient in left lateral decubitus moving abdominal mass away from the midline
Utilise lower frequency probe setting (turn to penetration mode) will help improve depth of penetration
Will lead to deterioration of image resolution
Machine has limited maximum depth of penetration
Use colour power Doppler to help identify aorta
Still provides information even if probe near 90 degrees incidence to the aorta
Will not show any directionality of flow
Use coronal windows as above
Often imaging of the aorta will be incomplete- if there is clinical concern about potential aortic pathology a CT scan should be discussed and considered with senior ED doctor advice.
PITFALLS AND MEASURING AAA
Measuring AN AORTIC ANEURYSM
Outer wall to outer wall
Include any aortic thombus in your measurements
Ensure maximal dimensions are measured
Ensure on plane measurements i.e. At the midline of the short and long axes of the aorta

Source: Core EM (Modified)
PITFALLS TO AVOID
Excluding an aneurysm on the basis of an incomplete ultrasound
If your ultrasound views are incomplete you cannot conclude a normal exam
No AAA does not exclude other aortic pathology - in particular dissection
An aorta > 3cm is abnormal
small aneurysm can rupture, interpret in clinical context
Not identifying the aorta correctly
Ensure accurate orientation and visualisation of both the IVC and aorta at the start of your scan
Measuring in a single plane
May miss eccentric, ectatic, or saccular aneurysms
May be difficult to visualise aortic anatomy in a single plane
Measuring only the true lumen of an aneurysm
Outer wall to outer wall including thrombus - best to over estimate